The
human
auditory sensory system, usually referred to as simply the Ear,
is a remarkably complex system that is usually taken for
granted by individuals with unimpaired hearing. It is the main
subject of study by audiology,
usually with an emphasis on speech perception and a variety of
hearing disorders. When we discuss the historical evolution of
these issues below, we will suggest that the modern concept of
"normal hearing" became defined at the point where
hearing ability could be quantified, around 1930, and since
then, audiological measurement has determined what that meant.
An audiologist specializes in the study and treatment
of hearing impairments (and usually has a Master’s degree),
whereas the measurement of hearing ability is termed audiometry
and is practiced by a audiometrist who gives what is generally
called a “hearing test” and can recommend hearing aid
equipment. Due to the rapid evolution of digital hearing
aid technology today and the ongoing development of cochlear
implants, we will leave those topics aside for the time
being.
The branch of medicine that is involved with the ear is called
otology,
and is usually included with otolaryngology, commonly
practiced by an ENT (ear, nose and throat) doctor, who can
also be a surgeon. Note that the prefix "oto" (from the Greek
word for ear) always refers to the auditory system.
These professional branches associated with the subject of
hearing involve a large body of research knowledge,
particularly in comparison with what typical public education
teaches in schools. Here we can only summarize some of the
most relevant terminology and issues that are involved.
homeA. Anatomy of the ear. The
anatomy of the ear is commonly divided into three parts, the
outer, middle and inner ear as shown in this diagram.
The outer ear consists of the auricle, which funnels
sound waves into the ear canal, a process that we described
earlier as kind of impedance
matching
operation since acoustic energy does not easily pass
from open air to a small “tube”. Also when we discussedbinaural hearing,
we pointed out that the ridges of the outer part of the ear,
called the pinna (Latin for "wing" with the plural
being pinnae), create small delayed versions
of the sound wave. When combined with the direct sound,
these delays colour the spectrum above 8 kHz and provide us
with directional cues for front-back distinctions, as well
as elevation. The auricle and pinna are different for each
individual, and can change throughout one's lifespan.
The slightly curved ear canal (or “external auditory
canal”), as with any small enclosed space, provides a high
frequency resonant boost, as will be shown below. It ends at
the eardrum (or tympanic membrane) where the
pressure variations in the auditory canal cause it to
vibrate.
Care needs to be taken not to allow a wax
buildup in the ear canal, and sharp objects have to be
avoided. Even using a Q-tip is not recommended, and may
simply push the earwax (also called cerumen) deeper
where it can become impacted. A healthcare provider may
recommend liquid drops or perform an irrigation of the ear
canal with water, or a dry microsuction.
Foam earplugs are designed to be flexible enough to
fit into the ear canal, but custom-designed earplugs made
from other materials (preferably with flat frequency
response) can also be purchased. Noise-cancelling headphones
are now often used by the public, the principle of which is
described in the Sound-Sound
Interaction module. These types of protectors are
called ear defenders, and in the best cases, they
can reduce sound levels by 30-35 dB.
The pressure on either side of the eardrum is assumed to be
equal, but when the external atmospheric pressure changes
(as with elevation), there can be an imbalance in
pressure, most easily relieved by yawning (or
“popping” one’s ears). As you can see from the diagram, the
Eustachian tube leading to the lungs is what allows
that to happen. However, there is also a danger of infection
in this closed region beyond the eardrum, particularly with
high fever (childhood) illnesses such as German measles and
meningitis that can cause serious and even permanent damage
to hearing.
Autophony refers to hearing one's
own voice too loudly through the occlusion of the ear canal
by earwax or other blockage (similar to wearing earplugs).
It can also be caused by otitis media in the middle
ear (described below), or a disorder in the Eustachian tube
(Patulous Eustachian Tube) where it is sometimes open
and allows internal sounds to be conducted to the middle
ear.
The movement of the eardrum at the threshold of hearing is
said to be so small that it cannot be seen with the naked
eye as the distance is less than a wavelength of light. And
if it were any more sensitive, molecular movement could
heard! Given that it can also withstand pressure that is a
million times stronger (admittedly with discomfort) this
represents a remarkable dynamic range. However, very large
pressure transients can perforate or burst an eardrum,
though in some cases this can be surgically repaired.
The middle ear consists of three
very small bones (the smallest in the body) called the ossicles.
Their function is to transfer the energy from the eardrum's
response to changes in air pressure through these solid
bones as a kind of amplification (up to 22 times their
original amplitude) and deliver it to the inner ear. The
bones are commonly called the hammer, anvil
and stirrup because of their shapes, but their
proper names are the malleus, incus and stapes,
respectively.
In the above diagram, the very small stapedius muscle
(about 1 mm in length) which is attached to the stirrup, is
not shown, but its function is to damp a large
incoming pressure surge (greater than 85 dB) as a form of
hearing protection. However, for the brain to detect such an
increase and send a message to this muscle to contract
requires a time lag estimated at up to 300 ms. Unfortunately
this mechanism cannot react quickly enough to protect
against impact sounds with very fast attacks,
particularly gunfire, but also some other mechanized sounds,
in which case hearing protection must always be used.
The stapedius muscle can also be activated by one's own
speaking voice in order to prevent its low frequency
components (that become obvious with earplugs) masking other
incoming sounds.
Inflammation of the middle ear is called otitis media
and can be very painful and often affects young children.
As mentioned above, both the unimpaired
outer and inner ear have their own resonant frequencies, as
shown here, both in the range of 1-4 kHz. Together they give
a 10-20 dB boost to those frequencies prior to entering the
cochlea. This explains why the frequency response of the
ear, as shown in the Equal
Loudness
Contours, is always higher in the 1-4 kHz
range, at all intensity levels.
Frequency
response of outer and middle ear (source: Brüel)
The last bone in the ossicular chain is
the stapes, or stirrup (less than the size of your
smallest fingernail), and it acts like a piston at the oval
window of the cochlea (see the first diagram),
transmitting the vibration to the fluid inside. This wave
passes through the spiral-shaped cochlea as
described in the next section, with the round window
at the far end responding to the pressure that it exerts.
A small wave called otoacoustic emissions can be
emitted from the oval window and pass back through the
middle ear and out the ear canal where they can be picked
up by a microphone. They are a sign that the cochlea is
functioning properly.
Any impairment in the energy transmission through the
outer and inner ear results in conductive hearing loss,
which can be a mechanical issue caused by calcification of
the bones that can be corrected by micro-surgery, or by a
tumour. This transmission through the ossicles should not
be confused with bone conduction, which refers to
sound passing through the bones of the body and reaching
the cochlea (which is embedded deep within the bones of
the skull) as discussed next.
The inner ear consists of the
snail-shell-shaped cochlea
(cochlea is Greek for snail), the three semi-circular
canals and the auditory nerve passing to and
from the brain. Whereas the sound wave changes media from
the air, through the bones of the ossicles, and then to
the liquid filled cochlea, it is the analysis of
the wave inside the cochlea that is crucial – and the most
complex part of the system – so we will devote the next
section to understanding how it works.
However, before we do that, it is worth noting the
function of the three semi-circular canals, named for
their horseshoe shape, that are part of the bony labyrinth
of the cochlea. They are our balance mechanism,
each of the three responding to movement in the x, y and z
planes, that is, the three dimensions of possible head
movement.
The three canals are filled with endolymph,
similar to the cochlea, which responds to movement and
acceleration by bending the cilia of the hair cells,
also similar to the cochlea. The horizontal canal
detects motion when we turn our head left and right,
around a vertical axis. The superior canal does
the same for nodding the head around the lateral axis, and
the posterior canal reacts to a movement of the
head towards the shoulder. In other contexts such as
flying, these movements are called pitch, roll and yaw. It
is important to keep in mind that hearing and the
sense of balance are intimately connected.
B. Auditory analysis in the inner
ear. The interior structure of the bony cochlea is
tricky to understand because it includes a canal filled
with perilymph (a fluid similar to plasma and
cerebrospinal fluid, rich in sodium and poor in
potassium). This canal is called the vestibular
canal (scala vestibuli), that starts at the
base of the cochlea and the oval window where the stapes
is creating a pressure wave. This canal ascends to the
apex of the cochlea, spiralling around 2-1/2 times, and
then the wave returns down a second canal, the tympanic
canal (scala tympani), back to the basal
end where the round window is located to relieve the
pressure.
In between the two canals is the cochlear duct (scala
media), filled with endolymph (a unique
kind of fluid rich in potassium and low in sodium, the
opposite of the perilymph), within which resides the organ
of Corti which is attached to the basilar
membrane that separates it from the tympanic
canal. A similar membrane called Reissner’s membrane,
separates the cochlear duct on the other side, from the
vestibular canal. Given the spiral shape of these
canals, it is difficult to visualize them, but we will
try to do this with two cross-sectional diagrams. You
can also look for some of the digital animations of the
cochlear structure that are available online.
The organ of Corti was
discovered by an Italian anatomist, Alfonso Giacomo
Gaspard Corti in 1851. However, the hair cells attached
to it cannot be seen in visible light with a microscope,
and so it remained until the advent of the electron
microscope to make these features visible. In the
next diagrams, we can see more of the placement and
structure of the organ of Corti on the basilar membrane,
including the three rows of outer hair cells,
and one row of inner hair cells, all of which
can fire in response to the incoming sound wave and send
those impulses via the auditory nerve to the brain.
As you can see, the organ of Corti will move in response
to the fluid wave that affects the basilar membrane, on
its way down the tympanic canal. However, the hair cells
are not in contact with that membrane (which would
likely result in some damage over time). Instead, they
have contact with the tectorial membrane above
the cells, which is protected from the two canals and
the motion of the fluid wave.
As we have discussed previously in
terms of the spectral analysis along the length
of the basilar membrane – often referred to as a
“bulging” of the membrane, but better understood as an
oscillatory motion shown below at the right – there is
what is called a tonotopic mapping of the
frequency response along the basilar membrane according
to position along its length. If the membrane were
uncoiled, its length would be 33-34 mm –
incredibly small – with the position of resonance going
from high frequencies at the basal end to low
frequencies at the apical end, as shown.
Notice that the high frequencies are analyzed near the
base where the basilar membrane is the stiffest (thereby
allowing only high frequencies to resonate), with 4 Khz
at the first “turn” of the spiral. It is thought that
the mechanics of the fluid vibration in this area might
contribute an answer to the naive question: why do we
lose high frequency sensitivity with age, and not low?”
There are, of course, many factors involved in hearing
loss that we will look at in the next section, but it is
useful to keep this in mind.
The more important aspect of this
spatial arrangement is that the resonances at octave
intervals are equally spaced along this length, as
shown here. This gives rise to the logarithmic
scaling of frequency that we associate with cochlear
analysis. This diagram shows the octaves of the pitch A,
which double in frequency, as resonating at equal
distances from the base of the cochlea.
Frequency
distribution along the length of the basilar
membrane showing its logarithmic basis
When stimulated with a periodic sound,
the hair cells will fire at the same rate as the
periodicity, as long as it’s in the low to mid range
where there is time for them to regenerate. This ability
results in our fine-tuned sensitivity to pitch in those
ranges. Above that, groups of nearby hair cells will
fire together at the same cumulative periodicity, called
volley
theory.
We are now ready to examine the hair
cells themselves. A healthy ear has over 15,000
such microscopic fibres, which are actually bundles of
fibres called stereocilia, plus a singular one
called a kinocilium.
There are three outer rows of hair cells in a
V-shaped formation. They respond to lower intensity
sounds by being displacement sensitive.
They are shown at the bottom in an electron microscope
photo at the right. Above that is a diagram that shows
what “displacement sensitive” means in terms of
directionality – a full amplitude range signal is
produced when the displacement is to the right, as in
the top diagram, and zero amplitude when it is 90° away
from that direction, with a proportional diminution in
between.
The function of these outer hair cells
(found only in mammals) is to amplify quiet sounds,
such that a wider dynamic range of amplitudes can be
accommodated by a smaller range of hair cell
deflections, a process called cochlear amplification.
They also improve frequency discrimination which
is very important in speech and music. A chemical
reaction here also allows cells to adapt
to constant level sounds, since the brain is always
alert to new information coming in. On the other hand,
the outer hair cells are unfortunately also the first to
be damaged by noise, as discussed later.
In contrast, the single inner row of hair cells
responds to higher intensity levels, and their
stimulation is velocity sensitive.
You have probably thought of the hair cells as only
sending impulses to the brain along the auditory
nerve. This “ascending” pathway is referred to as “afferent”
and is well understood. However, the hair cells also receive
impulses from the brain along the “descending” pathway,
referred to as “efferent”.
These efferent stimulations are less well understood,
but in general they influence the behaviour of the hair
cells in terms of their response, such as in noisy
contexts. The ability to detect signals in a noisy
environment is well known to decline with age, for
instance. They can also modulate cochlear amplification
in the outer hair cells, mediate selective attention,
and create an improvement of the signal to noise ratio.
This also allows them to support adaptation
and frequency selectivity, which shows that the auditory
system is a dynamically functioning system, not
merely a passive signal processor.
C. Hearing loss and impairment.
Instances of hearing impairment have certainly
occurred throughout history, but it began to be
regarded as a serious medical and social problem in
the 19th century as a result of industrialization. In
fact, one of the early terms for hearing
loss was boilermaker’s
disease, because of the high sound levels
involved. However, many industries, particularly in
Scotland and the industrial north of England were
known to produce serious degrees of hearing loss, as
in the well documented case of the female jute weavers
that will be discussed shortly.
Although noise has been and remains a significant
cause of hearing loss (referred to as NIHL,
Noise-induced Hearing Loss), there are many other
causes and types of degradation of the auditory
function, such that it is regarded as a worldwide
problem, estimated as affecting over a billion people
in various degrees. We will start by giving a brief
summary of the major types of hearing loss, and
associated issues.
These conditions should be kept separate from deafness
(or anacusis) which is a complete lack of
hearing ability, with an associated community who have
established their own forms of communication such as
sign language. The "hard of hearing", on the
other hand, are those who use a mix of lipreading and
hearing aids.
We will provide brief definitions
first, and then discuss some of these categories and
conditions more fully. Note that all of them can be
unilateral (a single ear) or bilateral (both ears),
asymmetrical (affecting each ear differently), and
experienced in combination.
- acoustic
trauma refers to a sudden and severe sensorineural loss
of hearing (over 40 dB loss), often incurred by a
single exposure to high sound levels, for instance
from an explosion or gunfire, or very high levels over
an extended period; the aftermath of the trauma can
include ringing in the ears (tinnitus), balancing
problems, and hyperacusis,
a painful sensitivity to certain frequencies or
sound levels which often affects musicians (and may
accompany other diseases)
- conductive
hearing loss, as referred to above in terms of
the transfer of acoustic energy through the outer and
inner ear; the causes are quite varied but often can
be treated
- sensory-neural
(or sensorineural) hearing loss, which refers to
a gradual reduction of hearing sensitivity in the
cochlea through damage to the hair cells; it can be
temporary (that is, recoverable with rest and quiet),
chronic or permanent, and is measured with an audiogram,
as shown below; it can also be sudden as described
above as acoustic trauma, and can be combined with
conductive loss
- central
hearing loss, which refers to an impairment
resulting from defects in the central nervous system,
including the auditory cortex, rather than the middle
or inner ear; it can be caused by lesions in the
auditory pathway or cortex such that sounds are heard
but not understood
-
presbycusis
is age-related hearing loss, always in the high
frequencies, and has many contributing factors, as
discussed below
-
tinnitus
refers to a persistent sound in the ears when there
is no external source; it can be a byproduct of
ototoxic chemical exposure or excessive noise, or it
can be an indicator of other medical problems
-
recruitment
is a non-linear amplification of sounds where normal
level sounds are heard as much quieter, but above a
certain point, they are heard as much louder, and
therefore they can mask other sounds and create
sensory-neural hearing loss; the non-linear gain
with this condition is similar to hyperacusis,
mentioned above
-
diplacusis
is a loss of frequency sensitivity in one ear that
results in pitch being heard differently in each
ear, sometimes called double hearing or interaural
pitch difference; based on an appreciable delay
between the ears, it can also affect rhythm
perception
The sources of hearing loss are often
divided as follows:
- occupational
hearing loss is associated with workplace
exposure to noise, for which most industrialized
countries have established damage
risk
criteria (discussed below) and other regulations
- sociocusis
is non-occupational hearing loss, and thus harder to
regulate; it also makes it more difficult to
adjudicate occupational claims for compensation
because the measurement of hearing loss cannot
distinguish which sources are its cause
Sensory-neural hearing loss. A
standard hearing test – which is now usually offered
free of charge at most audiology clinics – includes a
pure-tone audiometric test and a speech-in-noise test,
given to each ear separately since their sensitivity can
be quite different. In fact, bilateral differences are
quite common.
It may also involve other tests, such as with a typanometer
that sends a puff of air to the eardrum to measure its
responsiveness, to test if there is any conductive
hearing loss. Other tests may involve the cochlear
response.
The results of the pure tone tests (i.e. sine
waves) for frequencies, usually between 250 Hz and 8 kHz
(known as the speech range), are displayed on a graph
called an audiogram.
Note that the threshold of hearing level is at the top
on the 0 dB line. This line has been flattened out to
account for the threshold of hearing being variable at
all frequencies, as shown on the Equal
Loudness
Contours.
The vertical axis is called the Hearing Level in
positive dB increments (which is referred to as dB
HL), and indicates the signal level above
the threshold that the subject has been able to just
detect. Values for the left and right ears are plotted
separately, and together they show the frequency
response of the ear.
An audiogram
showing the typical notch at 4 kHz associated with
noise-induced hearing loss
Values above the 0 dB hearing line are possible for
unimpaired hearing, either because of the standard
deviation of the measurement (+ or - 5 dB) and the fact
that when the test is being done, it may be difficult to
determine which is the faintest sound that can be heard
(with multiple exposures being required and an average
taken of correct responses).
Low frequencies below 250 Hz are not
usually measured because there is seldom any hearing loss
(HL) in that region, and those frequencies are not
important for speech. Likewise there is no test above 8
kHz where the amount of presbycusis could be
detected, again because of a bias towards the speech
frequencies, ignoring their role in music, and
environmental sound localization. In fact, until recently,
audiologists have only focussed on speech perception and
therapeutic interventions aimed at its improvement.
One advantage of the graphic format of an audiogram is
that it shows hearing loss as a vertical decline
(compared with other graphs we will present below), and
therefore the results are communicated more intuitively.
"Normal" hearing is regarded as the range from -10 dB to
+15 dB HL, with the range of 16 - 25 dB being a slight
loss. A hearing loss of 25-40 dB is regarded as “mild”,
40-60 dB as “moderate”, even though this degree of loss
will create serious problems in communication, and below
that, “severe” and “profound” loss, the latter being
deafness. The complete scale is shown here.
Degrees of hearing loss shown in dB HL (Source:
healthyhearing.com)
Another important role of the audiogram
with NIHL (noise-induced hearing loss) is that it
clearly indicates the effects of noise exposure, which are
quite distinct from presbycusis (age-related HL). The old
excuse that HL is just because of age, and not noise
exposure, is untenable. NIHL occurs with a characteristic
notch
at 4 kHz, as shown above, and typically deepens on the
lower side over time. As we have repeatedly seen throughout
the Tutorial, this is the frequency range that is most
important for speech
and other essential aspects of acoustic communication,
particularly because it incorporates both vowel and
consonant information.
Here is a sound example where we implement the same severe
loss shown in this particular audiogram shown above. Note
how muffled and ambiguous the speech is, even on headphones.
If significant background noise were present, the
intelligibility would be even less, as dicussed below.
Voice
heard without and with the hearing loss shown in the
audiogram above (Source: Sylvi macCormac)
Temporary Threshold Shift (TTS)
shows the same notch pattern in an audiogram, as in the
diagram below, on the left for workers at the start and end
of a shift, and at right for a rock band rehearsing or
performing for three hours at a very dangerous level of 112
dBA. In fact, as discussed below under Damage-Risk
Criteria, any exposure above 90-95 dBA for
this length of time is regarded as having a high risk of
permanent hearing loss.
TTS is the result of the outer hair cells (those
that respond to lower levels of sound) becoming saturated
and are no longer firing. They are also deprived of a
nutrient supply of blood via the very tiny capillaries that
service them. One effect of noise, as we will see in the
next module, is an increase of blood pressure and decrease
in blood flow to the “extremities” which normally means the
hands and feet, but it can also affect the hair cells and
the semicircular canals for balance.
It should also be noted that, whereas TTS as a formal
definition refers to noise exposure, there are other
conditions, such as even the common cold or earwax buildup,
that can reduce hearing acuity on a temporary basis. As
discussed in the Magnitude
module, hearing is constantly adapting to the ambient
sound level, such that our impressions of loudness are relative,
not absolute. We are generally unaware of these shifts,
unless we go from a relatively high to low ambient
situation, or vice versa.
The key difference is that TTS puts the emphasis on a change
that may become permanent, unlike this continuous change in
hearing sensitivity that we experience every day.
19. Personal Listening
Experiment. Buy a pair of foam
earplugs at a drugstore (they are good to have on
hand), make sure they are fitting snugly in your
ears and are comfortable. Leave them in for at least
a half hour, or longer if possible, as you go about
some daily walking activities (but not driving or
biking). What sounds become magnified, and which
sounds that you normally expect become muted or
absent? When you eventually remove the plugs, you
will have a threshold shift where everything will
sound louder than normal. Estimate how long it takes
to adapt to the ambient level where you are. The
effects you experience are based in the occlusion
(blocking) of the ear canal, and increased awareness
of bone
conduction.
Sometimes
audiologists and others, trying to explain TTS, use a
comparison to trampled grass which can “recover” if not
walked on further. Admittedly, the stereocilia of the hair
cells might be comparable to grass, but the cause of TTS is
not a physical one of being crushed. Overstimulation and a
lack of blood supply is a better explanation.
Another side-effect of more severe noise
exposure is a ringing in the ears, called tinnitus,
which is caused by the hair cells firing spontaneously
after the overstimulation. This should in fact be an “early
warning signal” that over-exposure has occurred and future
exposure should be avoided. It can also occur as a
side-effect of, most commonly, aspirin and similar pain
management drugs which also constrict the blood vessels and
reduce flow to the hair cells. However, there are many other
causes of tinnitus as noted below.
If there is insufficient time for recovery, TTS can become chronic,
and eventually a permanent threshold shift (PTS). If
this is the result of noise it is called NIPTS
(Noise-induced Permanent Threshold Shift). PTS and NIPTS
mean that some of the hair cells are dead and, as is typical
in mammals (but not fish or birds), they cannot be
regenerated.
These graphs, generated from lab experiments, show that
there will be approximately a 25 dB TTS after an hour’s
exposure to a 4 kHz noise at 90 dB, and the shift will be in
the range of possible acoustic trauma (leading to PTS) after
8 hours. The righthand diagram shows recovery times
for a full 7 days of exposure which will lead to PTS.
However, the dotted line shows that a 95 dB exposure for
just under 2 hours will require a full day for recovery.
This indicates how noise exposure can become chronic if
there is not at least 16 hours of non-exposure, and result
in permanent loss of course with higher levels.
The Jute Weavers. The long-term
effect of NIPTS, as to how it keeps worsening, has been
well established since the original publication in 1965 of
the case of the “jute weavers” and their audiograms. What
has not always made clear, is that these were all women
who had worked in the mills of Scotland for anywhere from
1 to 40 years in a constant, high intensity level factory
setting measured at around 100 dB, without hearing
protection.
The sad truth about their existence is only mitigated by
the contribution the knowledge of their plight has served
for audiology. The clarity of the data was supported by
the fact that these women had little or no exposure to
gunfire, or other high level noise other than their
workplace. And most had never worked anywhere else, so the
cause and effect paradigm was near “perfect”.
Audiograms
for the jute weavers after multi-year noise exposure
The curves from top to bottom, then left to right, show that
the sensory-neural HL in the first 10
years keeps growing around the 4 kHz notch, but after that,
it starts digging more deeply into the 1-3 kHz range – all
of which are important speech frequencies. The old excuse
not to wear hearing protection in older workers (because
their hearing was already gone) is not valid.
The data also suggests why the relatively
slow but steady deterioration can lead to denial and some
forms of adaptation by the worker’s family and friends. Lipreading
will likely be practiced more, friends and family may learn
to “speak up” (even though it’s clarity, not loudness that
matters), but in the end there is greater social isolation.
Most of us have no experience, luckily, of working in such a
high intensity industrial situation, and in developed
Western countries such conditions would not be allowed
without hearing protection. But in the rest of world, there
are usually few such measures being enforced. Here is a
recording made in a German textile manufacturing factory of
a room with 100 weaving machines whose output was measured
at 100 dBA, similar to that of the jute weavers. This
excerpt only lasts a minute, but if you have a Sound Level
Meter and turn up the volume to even 90 dB you can
experience how intolerable the loudness of the sound is.
Ironically, since the recordist was moving about the room,
it has been commented on that the rhythms of the machine are
aurally interesting.
100 weaving machines at 100 dB, Kolb & Schüle textile
factory, Bissingen, Germany
Source: WSP Eur 17 take 9
This next diagram is a graph that shows more or less the
same data, but in a reverse format in terms of the “growth”
of the hearing loss, which is less intuitive but still quite
telling. It shows that the 3 and 4 kHz loss occurs fairly
quickly over the first 10 years, and after that, there is
still steady growth at 1 and 2 kHz.
Lastly, we should clarify another myth
about sensory-neural hearing loss. Speaking more loudly to
someone with this kind of impairment is not the right thing
to do (and certainly no one likes be shouted at). It is
better to (1) face the person and allow them to lipread,
once you have their attention, and (2) to speak more clearly
and enunciate words properly.
The other implication of this kind of HL is that the person
will avoid noisy situations because they are less able to
pick out conversation and other sounds from the background
din. Over time, this tendency promotes social isolation. We
can try to understand the reason for both of these
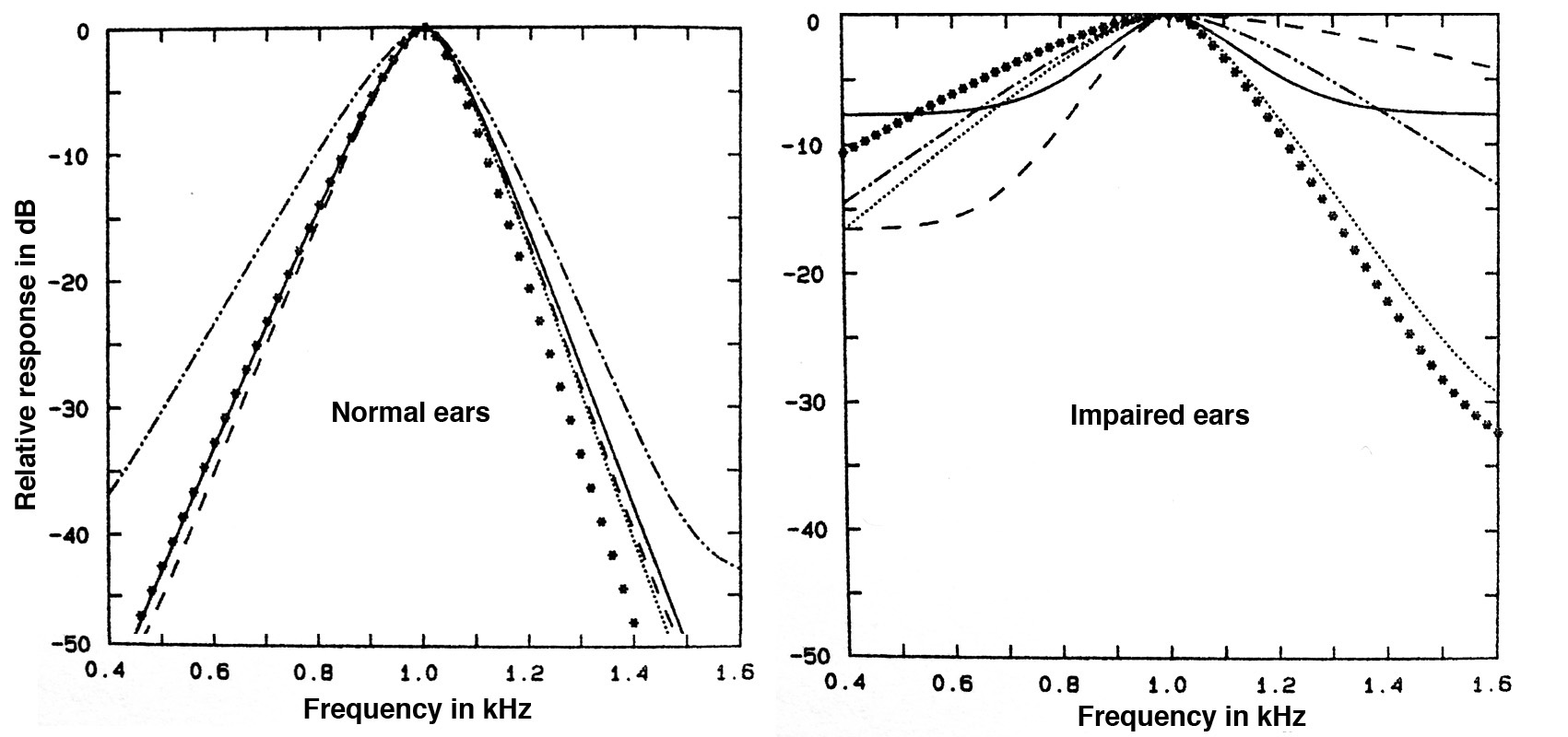
situations with the following graphs that shows how impaired
hearing (in different subjects) differs from normal hearing
in the frequency resolution of the ear.
Frequency
resolution
in normal and impaired ears at 1 kHz
The “normal” graphs for the 1 kHz centre frequency are sharp
and well defined. Therefore, information in adjacent bands,
and across the frequency spectrum, are more detailed via the
distribution of resonances along the basilar membrane in the
cochlea. For impaired ears, the filter bands are much
broader and even less well defined for lower frequencies
below the centre. Hearing with this type of reduced
sensitivity would be like seeing through a blurry window -
nothing would be well defined, and distinguishing a sound in
the presence of noise would be degraded.
Hearing loss, particularly with age, can also involve less
sensitivity in the time domain. A clear example of this, as
shown in this video,
is with the brief silences associated with the plosive
consonants. Lessened sensitivity to these brief silences, as
shown with the word "say" in this link, can lead to
difficulties in speech detection.
Presbycusis. The deterioration of
hearing with age is called Age-related Hearing
Impairment (ARHI), but it is also known as presbycucis
and regarded as a non-occupational type of loss. It
normally takes the form of a roll-off of high
frequencies above 8 kHz, similar to a low-pass filter,
with higher frequencies attenuated first, then progressively
lower ones with age. As we saw with the audiogram above, the
very high frequencies are not normally measured in a
standard hearing test, as they do not directly affect speech
comprehension. Speech and music with such a high frequency
roll-off merely sounds duller.
However, these diagrams show a typical presbycusis loss in
men and women for the critical speech frequencies of 1-4
kHz, according to age. The loss is always greater for men
than women? Why would you suppose that to be true?
Typical presbycusis curves for men
and women
in the most critical speech frequency range
If you answered the above question by thinking that men
would be more likely to be exposed to noise in the
workplace, that doesn’t fit the definition of presbycusis
which is non-occupational. Other gender specific factors are
more likely to be the explanation; for instance, female estrogen
has a protective effect on hearing. However, presbycusis can
also combine with the more common NIHL sensory-neural
hearing loss (with the 4 kHz notch) and can affect detection
of both the consonants and higher vowel formants.
There are many other factors in ARHI, such
as exposure to toxic chemicals, and various types of
medication that are ototoxic (i.e. damaging to
hearing), such as aminoglycosides, cisplatin, salicylate and
loop diuretics which are sometimes prescribed for older
people. Medical conditions such as diabetes, renal failure,
immune function impairment and cardiovascular disease may
also play a factor.
When we are considering a life-long set of factors that can
affect health, it should not be surprising that hearing
impairment with age is mainly correlated with overall
health, as well as noise exposure. Hearing loss is widely
thought to be “natural”, but it is more likely to be a
reflection of one’s overall health.
This type of question about presbycusis
being inevitable or not received a great deal of public
attention in the 1960s when the American otologist Dr.
Samuel Rosen studied a group of people known as the Mabaan
in the Sudan south of Khartoum. The environment was
essentially noise-free (with typical levels below 40 dB),
except during celebrations.
In Rosen’s autobiography he says that “they walked along the
trails single file, sometimes separated by as much as 100
yards, the length of a football field. Yet they conversed in
normal tones. The one in front did not even turn around to
reply!”.
Once audiometric tests began, he noticed much less high
frequency decline with both older men and women, including
testing the very high frequencies of 14, 16 and 18 kHz which
Western adults can seldom hear. But it was his remark that
“Mabaans aged fifty to fifty-nine had much better hearing
than Americans aged twenty to twenty-nine” that caught the
public’s attention through media reports. In fact for years
later, a general idea that “some African tribe didn’t lose
their hearing with age” still circulated widely.
One of the graphs in his research publication (in Transactions,
American Otological Society, vol. 50, 1962) did show this
comparison between the Mabaan men aged 50-59 and American
men aged 20-29 being similar, but the American data was Aram
Glorig’s 1954 Wisconsin State Fair data with noise-exposed
subjects, one of the worst set of findings ever reported.
However, to be fair, Rosen also showed a comparison with
non-noise exposed American men, also by Glorig (1960), in
this diagram.
Although
Rosen thought the noise-free environment of the Mabaan
played a role, he was more impressed by the fact that they
had low blood pressure that did not rise
significantly with age, as did American data. They also had
no incidence of hypertension, coronary thrombosis,
ulcerative colitis, duodenal ulcer and bronchial asthma. As
noted above, high blood pressure constricts the blood supply
getting to the hair cells, and therefore it is plausible to
regard that as an important factor in the lesser level of
ARHI among these people. It was also a good reminder that
everything involved in human health is connected, and we
should be careful about seeking single causes for any
health-related issue.
Recruitment. Auditory recruitment
is dysfunction of the inner ear that distorts the
dynamic range of the sounds being heard. Low level
sounds seem quieter than normal, but past a certain
threshold their intensity becomes magnified by a non-linear
amplification and they become overly loud. This
effect, which can be made worse with a hearing aid, means
that quieter sounds are masked and the person experiences a
threshold shift after each burst of loudness that is similar
to permanent hearing loss.
Non-linear dynamic response associated with recruitment
This diagram compares a normal dynamic response (dashed
line) which is quite linear, with a non-linear response
pattern typical of recruitment (solid line). For
instance, a 60 dB tone in the impaired ear was matched in
loudness to a 30 dB tone in a normal ear (basically turning
normal speech loudness into a whisper). Normal speech at 60
dB sounded with equal loudness as a shouted 80 dB, and so
on. This distortion can occur even at the phonemic level
where louder phonemes will mask quieter ones, making speech
very problematic to understand.
Here are two examples of a simulation of recruitment, taken
from an Australian Broadcasting Corporation documentary
called "The World of JK", about a boy who is referred to as
"deaf", but in fact suffers from recruitment. The first
simulation is of a normal dinner table event where familiar
percussive sounds and voices are distorted, and the second
is an audiological test for word recognition where the boy
is asked to repeat test words, first with no assistance, and
secondly where he is allowed to lipread his father mouthing
the words.
Simulation of how dinner conversation might be heard by
someone with recruitment
Simulation
of how a word test might be heard by someone with
recruitment, followed by the same test with lipreading
Tinnitus is the experience of a
persistent sound in one or both ears when there is no
external source. It is often described as a ringing,
buzzing, hiss or roaring. The term can be pronounced with
the emphasis on the first or second syllable.
Tinnitus is generally regarded as an indicator, not a cause,
of another condition, most commonly NIHL and presbycusis,
but it can also be a side-effect of many other medical
conditions as well. As noted above, a transient version of a
“ringing in your ears” (in the 5 - 10 kHz range) can be
experienced as a response to excessive noise exposure, or
medications such as aspirin which constrict blood flow, and
result in a spontaneous firing of the hair cells.
However, with various chronic diseases it can become a
nearly constant presence and therefore create psychological
and other problems such as depression anxiety and stress,
depending on its severity. It is estimated to affect 10-15%
of the population, and despite the search for some form of
medical relief, there are no proven medicines that can be
prescribed. However, a variety of therapies can be tried,
such as introducing sound to mask the tinnitus or distract
from it, and notching out frequencies close to the tinnitus
frequency.
Ototoxins in history. Chemicals
and drugs that have the potential to damage hearing have
been mentioned several times in this module. However, they
have a much longer history. Historian Hillel Schwartz’s
encyclopedic tome Making Noise (Zone Books, 2011)
documents the long history of noise (which his subtitle
alliteratively reminds us is “from Babel to the Big Bang and
Beyond”), and provides amazing detail about the Industrial
Revolution’s introduction of countless sources of noise.
However, he also points out that in the 19th century,
exposure to ototoxic chemicals (such as lead, mercury and
solvents) was widespread, high fever diseases were common
and produced hearing loss in both children and adults, and
that the medicines that were available (quinine, morphine,
cocaine in its alkaloid form, and by the end of the century,
aspirin), all of them could be ototoxic and result in
tinnitus, depending on the dosage (pp. 368 ff). So what if
anything constituted “normal hearing” at that time?
Audiometers and sound level meters were not invented until
the late 1920s and early 30s with the electrical
developments at Bell Labs that we have mentioned several
times. So, at that point of the ability to quantify sound
(and hearing), the modern concept of what was “normal” and
“impaired” began to be solidified. Likewise, noise abatement
measures began to be put in place, as documented for Europe
and North America by Karin Bijsterveld in her comprehensive
Mechanical Sound (MIT Press, 2008). However, damage
risk criteria for industry, at least in North America, had
to wait until the 1970s.
D. Damage-risk criteria. The
institutionalized approach to risk management usually
involves establishing risk
criteria and appropriate standards to guide
exposure. In North America, these criteria for the
workplace were slow to be adopted in terms of risk to
hearing, but in 1971 the Occupational Safety and Health
Act in the U.S. came into effect for noisy industrial
environments, to be administered by the OSHA (Occupational
Safety and Health Administration) in the Department of
Labor. As might be expected, the initial guidelines were a
compromise between industry, worried about costs, and
audiologists who were more concerned about aural health.
These first guidelines were stated as shown here.
The main two characteristics of the criteria were the
8-hour exposure limit (set to 90 dB, whereas
audiologists recommended 85 dB) and the “exchange rate”
of 5 dB increase for half the amount of time (whereas
audiologists would have preferred a 3 dB rate). There was
also a general reference to impact noise measured at peak
levels.
The other problem with this initial set of criteria is
that it was labelled as “permissible” levels, but
which were clearly not “safe” levels. In other
words, they did not guarantee a lack of occupational
hearing loss, as some might have assumed. Some
commentators have suggested something along the lines that
at these exposure levels, a hearing loss of no more than
15 dB would be experienced by 1/3 of those exposed.
A larger issue that has been raised by
some critics, such as Raymond Hétu from Québec, is that
this approach solidified hearing loss as the main basis
for regulation and compensation, as administered by
audiologists using audiometric methods. Given the range of
noise effects that will be outlined in the next module,
there are many more consequences of noise in the
workplace, many of which can increase the risk of
accidents, as in Hétu’s diagram here.
Outline of the
effects of occupational noise exposure (source: Hétu)
In more recent decades, there has been
a move by regulators towards hearing conservation
programs. This involves providing annual hearing tests
for workers (in medium to large business and industrial
operations), and prescribed levels of hearing protection
based on the time-averaged noise levels that have been
measured.
Many jurisdictions now follow the standard of 85 dBA
time-weighted exposure over 8 hours, and a 3 dB
exchange rate (that is, halving the duration of
exposure for each 3 dB increase in sound level, as
recommended by the NIOSH (National Institute for
Occupational Safety and Health). The aim is to reduce
the risk of occupational NIHL, and a comparison of OSHA
and NIOSH criteria is shown here. Note that the
time-weighted level Leq will be explained in
the next module.
The effectiveness of personalized
hearing protection is measured as a NRR value (Noise
Reduction Rating), although its actual
effectiveness depends on the fit and pattern of use by
the user. Some estimates show that actual use is often
about half of the maximum value. The following chart
shows how to calculate the estimated noise exposure
level using the NRR value, for earmuffs, earplugs and
their combination (“dual protection").
For instance, with a Leq of 98 dBA and a NRR
of 30 for earplugs, the estimated noise exposure is 80
dBA, with an effective rating of 50%. With earmuffs,
that value would be reduced to around 74 dBA (effective
rating of 70%). Of course these values assume an ideal
fit for the protection and 100% use.
The best protectors are the closed over the ear
headphone or earmuff type protectors (class A), with
soft foam earplugs or fitted plugs as class B if they
can reduce levels by 30 dB. It is important that the
reduction is fairly uniform across the entire range of
frequencies so that speech can still be understood,
given that high frequencies are easy to attenuate, but
low and mid-range ones are not. There are some
misconceptions about hearing speech or other signals
when using earplugs. Research shows that it is easier to
detect and comprehend these sounds when the ambience is
lower, particularly if all frequencies are reduced by
about the same amount, and therefore it is better to use
earplugs in those situations, as speech may be better
understood.
Impulse content of noise. The
criteria described above are solely based on a dosage
model, which is basically averaged noise level plus
duration of exposure. A dosimeter (or
"dosemeter" in the UK) is sometimes used, attached to
the worker’s clothing, to determine the dosage of the
exposure, a procedure that can easily produce a flawed
result as the worker moves about. However, under very
noisy conditions, that interference will likely be
negligible compared to the external sources.
Today, the Equivalent
Energy
Level, or Leq, can do a better
job and is incorporated into many portable sound level
meters and apps, and the averaged result can be measured
over any length of time. It is usually A-weighted (in
dBA) and therefore discriminates against low
frequencies, with the traditional justification that dBA
“reflects how we hear”, a non-technical reference to the
Equal
Loudness
Contours from which the A-weighting scale
was derived for low intensities (the 40 phon
curve) as described in the Magnitude
module. However, you can see a reference to dBC levels
in the chart above, which does include low-frequencies,
but that weighting network isn’t always available and
cannot be used in windy conditions outdoors.
On the other hand, it has been known for several decades
that industries where impulsive noise content is
prevalent, such as with a punch press, or in the impact
sounds made by glass and metal hitting each other, or
other types of mechanical operations, average risk
limits for 50% hearing loss are lower and therefore the
risk can be greater, as shown here from a report in the
1970s in Europe.
Risk limits for different industries with impulsive
content (source: Brüel)
Note that the lower the line, the higher the risk
because of impulsive content in the typical sounds of
that industry (that is, the risk of hearing loss is the
same at a lower level). It is a small comfort that
amplified pop music (which the Europeans call “beat
music”) is less risky because the audio equipment cannot
reproduce the brief transients that are the problem.
However, the same dosage model (level plus
duration) still makes amplified music as dangerous to
the ears as any other industrial noise.
What has not become generally integrated into risk
criteria today is the impulsive content of
sounds. Everything we have described so far relates to steady
noise levels. Admittedly the Leq measurement
will include the energy of brief transient sounds, but
it is not clear what time-scale should be used, as many
of these transients can last under 100 µs
(microseconds). In the following diagram, we can see
examples of these short transients in a beer bottling
plant. Note that the strongest spectral energy is in the
2-3 kHz range.
Spectrum and waveform from a bottling plant showing
brief impulsive transients (source: Brüel)
Of course, it has been long known that gunfire
of any kind can produce acoustic trauma
(permanent hearing loss) with even a single exposure,
and as described above, the stapedius muscle that has
the capability of damping an incoming pressure transient
in the ossicles, cannot do so fast enough to prevent
this kind of damage. Peak levels that can range from 140
to 175 dBA will cause permanent damage.
Traditionally, the sound level meter (SLM) has had two
settings for its temporal response, slow (for
visually averaging a time-varying sound with a 1
second averaging time), the fast response
for tracking rapid transient sound levels, and the
impulse response for peaks. The fast response of the
meter at 125 ms is closer to the brain’s own
averaging time, which also determines the apparent
loudness of a sound, as demonstrated in the demo with short clicks.
The impulse meter (now seldom used) has the time
constant of 35 ms. Instead, the C-weighted instantaneous
sound pressure level is often used with impulsive noise
such as a nail gun or drop hammer, but it is unclear as
to whether energy in the microsecond range will be
adequately assessed.
In fact, if you watch a SLM fluctuate on the fast scale,
it is easy to see the correlation between what you are
hearing and what is being measured. However, the danger
with impulsive sounds arises because there is nothing
preventing them from going directly into the inner
ear and causing damage. The averaging times for
the outer and middle ear are in the microsecond range.
Moreover, as documented above, the natural amplification
of the sound wave in the outer and middle ear is 10-12
dB, and as we just saw in the above diagram, that
frequency range is where most impulsive energy lies.
20. A personal listening experiment
for this effect (but don’t do it for very long) is when
you hear bottles hitting each other, or a series of
metallic impacts, or even hammering at close range. They
won’t sound that loud, but you can often feel an
after-effect of discomfort or a Temporary Threshold
Shift. If you have to work in such an environment, use
hearing protection!
Of even
greater concern is that some children’s toys, such as a
toy “cap pistol”, or fireworks, can also produce very
strong pressure transients.
A peak sound level measurement
represents the true maximum pressure of a sound wave, so
for instance, a sine wave’s peak (as opposed to its RMS
value) is 3 dB higher than its SPL (sound pressure level).
In a digital meter, there is no time weighting involved,
but keep in mind we are dealing with time values near the
sampling period (e.g. 20.8 µsec for a 48 kHz
sampling rate), so higher sampling rates will need to be
used.
In terms of damage risk criteria, there are some
guidelines about impulsive content, such as an upper limit
of 135-140 dB peak levels, but as yet, there is no
agreement on exactly how the true peak levels should be
measured and how the threshold of risk for hearing loss is
determined. There is also no satisfactory way of combining
the measurement of steady state noise with impulsive
content.