Harmony Kaelan Ráine
I am a Perfect Failure, Thank You
Abstract
The purpose of this essay is two-fold: firstly, to discuss how, through the failure of my health and physical capabilities (at the worst possible time), I managed to successfully complete both my Bachelor of Fine Arts and Master of Arts degrees. Although I despised the daily struggles and suffering caused by my physical impairments and chronic illness, I must begrudgingly admit that I was inadvertently provided with a research focus. More importantly, being too incapacitated to overanalyze every detail liberated me from some of my own self-sabotaging tendencies (my obsession with perfection, daunting self-criticism, and overwhelming need to live up to others’ expectations – all driven, of course, by my paralyzing fear of failure). It is in this way that my body’s failure to cooperate allowed me to produce artistic and written works that reflected my true creative impulse and authentic self. Secondly, I wish to share an excerpt from my Master’s thesis, “When Words Fail: The Communication of Pain through Art.” The document, which is a thesis on how pain may be communicated in the absence of language, illustrates how the notion of ‘failure’ must be reconceived as a catalyst for further research, learning, teaching, self-expression, and creative problem-solving, and mirrors my journey of enlightenment through failure.
Preamble
I have come to accept myself as a perfect failure. By ‘failure’ I mean that I am a continuous work in progress; someone who is flawed, imperfect, disabled, has exercised poor judgement and made mistakes and bad decisions (and will continue to do so); but also someone who is willing to learn from trial and error when things do not go as planned (hopefully sooner rather than later). As an insecure perfectionist, it was not easy for me to embrace this philosophy – in fact, a series of very unfortunate, stressful, and challenging life circumstances led me (forced me) to change my old habits, ask for and accept help, and realize that my failures were presenting me with opportunities to re-direct my life.
On August first, 2010 – just one month before beginning the final year of my Bachelor of Fine Arts degree, I suddenly became physically and painfully disabled. Since the final year of a BFA program consists primarily of physically demanding, studio-based work and I had completely lost all function and mobility in my left shoulder and arm, I was forced to seriously question my ability to finish my education. My final body of work (which was already well underway) was to entail a series of large-scale sculptures, which I could no longer hope to complete. I could not lift my hand any higher than navel-height, with no weight, in any direction. When I explained my situation to my faculty advisor, she hesitated for only a moment and then challenged to me to begin a new body of work and “do it disabled.” I began to research the work of artists who used their own pain as praxis, decided to change my medium, and embarked upon the production of a new project loosely modeled after the performative self-portraits of Frida Kahlo, Hannah Wilke, and Jo Spence. I cannot emphasize strongly enough how quickly this decision was made (partly as a result of my instructor’s support and confidence in my abilities, and partly because of the investment I had already made in my education and unwillingness to quit). I have been learning that it is these types of ‘gut’ reactions that propel us toward our greatest successes, even in the face of failure. Malcolm Gladwell (2000; 2005) is a strong proponent for ‘thinking without thinking’ or ‘thin-slicing,’ which, unlike mere impulsiveness, is intuitive; and claims that it is the belaboured, anguished, over-analysis of situations and second-guessing one’s first instincts that can lead even the most talented among us to fail.
I not only finished my degree on time, but with a well-informed body of work and top honours. I did not heroically ‘overcome adversity’ or ‘rise above’ anything in order to achieve success. I simply followed my gut, worked intuitively, took a risk (albeit a calculated one), accepted help, used all the tools I already had at my disposal, and changed my direction. The body of work that emerged from my own, flawed and unstable self is raw, authentic, and true; a much more compelling and successful project than I assume I would have created had my physical health not failed so miserably at precisely that crucial moment in time. Halfway through my Master’s program, I developed the same painful condition on my right side (not to mention a badly herniated disc in my neck); and when it came time to write my final thesis, I also found myself plagued by daily, debilitating migraines with aura (complete with intense nausea, vertigo, confusion, persistent tinnitus, intermittent vision loss, double vision, and transient aphasia, dysphasia, and dysgraphia). There was absolutely nothing I could do to change my medical situation, the neurologist was less than helpful to say the least, I was on a rigid deadline, and was working for a living. I became trapped in a chronic cycle of pushing myself to read and write, vomiting, passing out, and wallowing in self-pity. Finally, I accepted that the only way I could finish my degree was to write from a compromised position and straight from my lived experiences. Because trying to understand any concept, constructing every sentence, and every bit of organization it took to formulate the paper was a monumental mental battle for me, I had no choice but to let go of my chronic over-achieving and self-critical ways. The fancy academic jargon would be kept to a bare minimum; there would be no frills, no over-thinking, and no attempts to impress anyone. I knew all along that the end result would either be an A+ or an epic fail. In the end, I produced a rather exceptional paper and learned that it was not my disabled body and chronic pain that had been holding me back. My fear of failure (along with fear of rejection, ridicule, and criticism) and my aching need to live up to other peoples’ expectations, were the forces that had literally been paralyzing me – creatively, academically, personally, emotionally, and professionally – my entire life.
I know I could have written a technically superior paper had I not been derailed by a brain-crushing, body disabling condition; but anything I might have produced from the perspective of wellness would not have held the valuable insights I gleaned and emotional impacts I was able to convey had I not accepted myself as I am: irrevocably flawed – a perfect failure, if you will. The following is a revised excerpt from my Master’s thesis.
When Words Fail: The Communication of Pain Through Art
Introduction
Pain is cross-culturally ubiquitous and is a unifying element among living beings. Individual pain, however, is unique and extremely difficult to describe to others (Bending 2006; Cohen 2000; Kleinman, Das and Lock 1997; Jackson 2002; Melzack and Wall 1982; Morris 1991; Scarry 1985; Semino 2010; Tumini and Crouch in Sternudd and Tumini 2011). Cultural theorists assert that the more intense the pain, the less communicable it is in linguistic terms (Caruth in Obourne 2005; Detsi-Diamanti, Kitsi-Mitakou and Yiannopoulou 2009; Morris 1991; Scarry 1985; Selzer 1994) and point out the cruel irony that survivors must construct a narrative to tell an empathetic listener in order to recover from trauma (Laub in Meyers 1997). The communication of pain can be further complicated by the fact that witnessing the suffering of others – especially when there is an inability to help – is intolerable to many people, who turn away or do not want to listen; and this often includes medical professionals (Jackson 2002; Scarry 1985). Pain, then, fractures bonds between the suffering self and others (Bending 2006) and effectively silences the voices of those who may be able to offer the most valuable contributions to pain research – pain sufferers themselves.
This wide gap may be bridged through the use of art as a language by which to communicate pain in the absence of words. According to Susan Sontag (2003), “in contrast to a written account… a photograph has only one language and is destined potentially for all” (2003). More than just universally legible, visual imagery reaches viewers on emotional, subconscious, and intuitive levels rather than through parts of the brain that control rational and logical thought processes that might impede reception (Nyham in Levine and Levine 1999). Artistic expression can be empowering; but by appropriating and subverting the gaze, art can also move beyond its role in empowerment to become an essential tool for communicating the corporeal and emotional feelings of people rendered speechless by pain.
Communicating Pain
As eloquently articulated by Virginia Woolf: English, which can express the thoughts of Hamlet and the tragedy of Lear, has no words for the shiver or the headache... The merest schoolgirl when she falls in love has Shakespeare or Keats to speak her mind for her, but let a sufferer try to describe a pain in his head to a doctor and language at once runs dry (in Scarry 2009, 4).
Physical pain, on the other hand, “does not simply resist language but actively destroys it, bringing about an immediate reversion to a state anterior to language, to the sounds and cries a human being makes before language is learned” (Ibid.). Physical pain is further complicated when it becomes chronic, assuming a prolonged or permanent status along with the knowledge, for many chronic pain sufferers, that making a recovery or ‘overcoming’ pain may not be achievable. According to David B. Morris (1994), [many] people today find themselves in situations in which time and drugs fail to bring relief. Such pain may expand to fill the patient’s entire consciousness and to create permanent disability. Quality of life measurably plummets. Indeed, a life filled with intractable pain is not just arduous and fundamentally disordered but very likely pathological (14).
Evidence suggests that the outward expression of pain is a physical necessity; however, pain silences sufferers through various processes – from the shattering of verbal language that results from intense trauma to socio-cultural taboos proscribing “the candid discussion of pain, illness, and natural death” (Fox in Sternudd and Tumini 2011, 17), to an overall lack of empathic witnessing. Moreover, psychological and emotional traumas that are not adequately processed have the potential to turn inward and later manifest in the body as physical pain (Ahmed 2004; Jackson 2002; Morris 1991; Wall 2000). Acute physical pain that is not treated in an appropriate and timely manner can turn into chronic pain that becomes resistant to treatment and causes long-term suffering (Jackson 2002). Research from across disciplines affirms that individuals in pain very often suffer in silence, are dismissed, misunderstood, marginalized, oppressed, and excluded from full social and economic participation (Cohen 2000; Jackson 2002; Thomson 1997; Wall 2000).
Painful conditions that cannot be verified through diagnoses (notably back pain, headaches, migraines, neuralgias, fibromyalgia, and chronic fatigue syndrome) pose the most serious challenges to communication; and even when an illness or injury can be clinically diagnosed, the feelings associated with pain are purely subjective and non-quantifiable. Despite a wealth of technological advancements, the inability to visualize and document the subjective experiences of pain leaves many sufferers feeling disbelieved and invalidated (245). Scarry (2009) notes,
if the only external sign of the felt-experience of pain (for which there is no alteration in the blood count, no shadow on the X ray, no pattern on the CAT scan) is the patient’s verbal report (however itself inadequate), then to bypass the voice is to bypass the bodily event, to bypass the patient, to bypass the person in pain (6-7).
Acute physical pain poses far fewer communications challenges to sufferers than chronic pain, not necessarily because it is less ‘painful’ or less traumatic, but because its source is often visible or can otherwise be referenced and understood. Acute pain is also often less distressing and less frustrating than chronic pain because it is perceived to be temporary, manageable, and recoverable. Morris (1994) argues, “we know what to expect from acute pain: It comes, it goes, it follows the rules” (8).
Frameworks by which to study pain are closely aligned with those used utilized in disability theory: namely, the individual / biomedical model (founded in modernism), the social model, and the cultural model. The individual / biomedical model has increasingly become the subject of intense scrutiny, primarily because of its tendency to diagnose, label, identify differences as pathological (Lewis in Davis 2006: 340) or as medical issues in need of medical solutions (Burns 2009: 21), and to medicate. The paradigm also notoriously reinforces paternalism and other power hierarchies by assigning the authoritative truth of the patient’s condition, including the veracity of pain, to the discretion of the medical institution (Ibid.). The wide acceptance of the gate-control theory of pain (developed by Ronald Melzack and Patrick Wall in 1962) led to the evolution of the social model, which acknowledges the role of social factors in disability, and the newer ‘biocultural’ model, which relies upon medical knowledge about nociception while acknowledging that “pain is never entirely a matter of nerves and neurotransmitters but taps into our emotional, psychological, and cultural experience in ways deeply entangled with the meanings we make or inherit” (Morris 1994, 15-16). Postmodernism ushered in cross-disciplinary and interdisciplinary paradigms wherein pain is now studied from the perspectives of medicine, bioethics, nursing, biology, pharmacology, psychology, sociology, social work, anthropology, art, visual culture, philosophy, feminism, queer theory, Marxism, critical race theory, identity politics, postcolonial theory, and deconstructionism. Biosocial and biocultural models also represent a vital postmodern shift that returns authority and control over the narration of pain, disability, and illness from medical personnel to the individual. The preponderance of internet chatrooms, forums, and blogs used by people in chronic pain represent some contemporary examples of the many ways in which pain sufferers have been finding their individual and collective voices and are claiming or reclaiming their agency through research, dialogue, and mutual support (Fox in Sternudd and Tumini 2011, 18). Because not everyone has access to verbal or written language (or has computer literacy), and because pain shatters language, the need to investigate alternative methods of communication remains urgent.
Toward a Universal Language
Since the introduction of Melzak and Torgerson’s ‘McGill Pain Scale’1 in 1971, a variety of rating systems has emerged for use in health care settings in order to try to understand patients’ pain. Clinically developed scales, however, are impersonal, tend not to ask open-ended questions, and cannot be viewed as true reflections of patients’ intimate feelings. Such methods also tend to rely upon basic literacy skills and knowledge of the dominant language. Rating scales that purportedly interpret facial clues, body language, heart rate, and blood pressure may be used with infants and people who are non-verbal, illiterate, have learning difficulties, dementia, or are unconscious; but every aspect of these scales is reliant upon the judgement of the test designers, administrators, or interpreters. Pictorial rating scales can offer a reasonable alternative in some cases, but the accuracy of any pain scale cannot realistically be determined because pain is subjective and relative, and because individual responses to both pain and visual stimuli are immensely variable (Jackson 2002).

Art Therapy, Art as Therapy, and Art as a Visual Language
“[Every] individual, whether trained or untrained in art, has a latent capacity to project his inner conflicts into visual form” (Naumburg 1987, 1).
It is important to distinguish art therapy and art as therapy from self-generated artistic expression used as a form of communication. In traditional art therapies, which are initiated and guided by a third party, art is used as a means by which to tap into repressed memories that have been too painful to recall. This process does not imply that one’s memories will be outwardly communicated to others, nor does the art specifically depict a sufferer’s pain. By contrast, the articulation of pain through performance art and self-portraiture represents conscious and purposeful efforts to illustrate and describe an individual’s perception of his or her specific pain sensations to others. The process may or may not generate cathartic release or feelings of empowerment. In fact, the opposite effects may occur.
The Representation of Pain though Self-Portraiture
Trauma, suffering, and pain have been consistent themes throughout the history of art, and a major paradigm shift occurred when groundbreaking women and feminist artists began to use images of their own bodies in pain in order to claim and subvert the power of the gaze (Devereaux and Hillman 1995; Jones 2002; Mulvey 1989; Sturken and Cartwright 2009). Pioneering artists like Frida Kahlo, Hannah Wilke, and Jo Spence, who chose to expose their personal pain publicly through self-portraiture, exemplify not only the effective use of art as a language for pain, but also that self-representation serves as a crucial act of resistance against the marginalization inherent in oppressive gazes. Positioning oneself as both the subject and object of an artwork deconstructs unequal power relationships. Therefore, exposing one’s pain, disability, illness, or non-conforming body disrupts normalcy through the purposeful embodiment and public display of corporeal differences as acceptable states of being. By taking control of the gaze and returning the viewer’s gaze through self-portraiture, the person in pain visibly and publicly assumes a position of power.

Figure 3: Jo Spence. Dated Self-Portrait from A Picture of Health? 1982-1986. Reproduced with permission from JoSpence.org

Figure 4: Jo Spence. Dated Self-Portrait from A Picture of Health? 1982-1986. Reproduced with permission from JoSpence.org

Figure 5: Jo Spence. Dated Self-Portrait from A Picture of Health? 1982-1986. Reproduced with permission from JoSpence.org
Disabled performance artists have maximized the politics of visibility and representation; and many cultural theorists now directly attribute the successful critique of eugenics and other forms of oppression to “the development of politicized disability efforts” (Snyder and Mitchell 2006, 4). Since the postmodern body is conceived as the ultimate site for the production and communication of cultural meaning, the disabled body or body in pain is crucial as a site of resistance and source of cultural agency (Ibid, 10). Disability theorist Rosemarie Garland-Thomson (2002) asserts that people with bodies that visibly “disrupt the expectations of the complacently normal [should] deliberately invite the stare-and-tell dynamic that constitutes... otherness” (335), quite simply because the person who initiates the stare “controls the terms of the encounter” (Ibid.). For people living in chronic pain or disability, staring is the political equivalent of the gaze (Ibid.).
Personal Interrogations – Officially Unapologetic (2011-2014): Is this Supposed to be Cathartic?
For me, the process of producing art that viscerally exposed my pain was not cathartic or empowering. In fact, it was emotionally draining, physically painful, and for a long time, felt pointless. As I worked diligently – impatiently awaiting the catharsis that failed to occur – I found myself becoming more and more frustrated, angry, and resentful about my life circumstances. While I waited for whatever ‘therapeutic benefits’ might be forthcoming from the documentation of my pain, though, I continued to learn from the process. Showing my images in exhibitions, receiving feedback on the work, and overhearing some of the comments made by viewers (who were most often unaware of my presence) reinforced my theory that images of pain are particularly arresting and engaging, and that such intimate works not only provoke fruitful and insightful dialogues and debates, but also have the capacity to promote a deeper understanding into the corporeal realities of people living in pain. I have also ascertained that because my work is purposefully ambiguous as to the nature of my pain, viewers feel at liberty to ‘read’ their own, often painful, narratives in the images. As a result, a form of creative, reciprocal witnessing often unfolds around such works, and a variety of dialogues can emerge from a single encounter with an image.
Of equal importance, the work has generated some negative feedback. The most surprising criticism came from my son, a successful young Vancouver-based videographer and filmmaker, who commented only that my work was “a visual assault.” My assumption had been that, as a fellow artist, my son would appreciate the work conceptually; however, when he reacted to the images with discomfort that bordered on revulsion (uncharacteristic for him given his aesthetic sensibility and the nature of his own work), I made two cursory hypotheses. Firstly, that responses to images of pain are highly conditioned by the lived experiences of the viewer (presumably that empathy, understanding, and acceptance are much greater among those who live in pain); and secondly, that responses to imagery of such an intimate nature are highly influenced by the type of relationship that exists between the viewer and producer of the work.
Another very important, unanticipated research finding was revealed to me while participating in an intensive anti-oppression workshop, wherein I learned the purpose and value of silent witnessing. As group members took turns enacting their personal pain, grief, or oppression through various wordless performative bodily gestures, others simply ‘held space’ for them, witnessing without comment or judgement. The underlying premise of all ‘body work’ is that physical, psychological, and emotional pain can become so deeply embedded into the self that the body manifests any and all types of pain as an integral part of one’s physical comportment.2 Thus, because pain becomes part of the physical body (often in ways that are imperceptible to others), it must be purposefully worked out through the body rather than through rational thought or verbalization. While having an empathic witness is important, expressing one’s innermost pain, whether through voice, art, or bodily gestures, has immense intrinsic value to the individual irrespective of external validation or the opinions of others (an audience is irrelevant to the process). These informally gleaned findings (as well as my own cathartic deprivation) led me to deeply ponder and question how, why, and for whom a work of art produces so-called ‘catharsis.’
During the course of conducting the research for my Master’s thesis, I stumbled upon Oliver Sacks’ (1992) Migraine, a condition with which I have suffered in a variety of forms since childhood. When, within its pages, I encountered graphic, visual imagery representing numerous facets of ocular migraine auras as well as art produced by migraine sufferers, the missing pieces of my research puzzle immediately began to slip into place. This is because the imagery spoke to me in a language that mere words could never express and led me to research migraine art. During my search, I discovered PainExhibit.org, a website that serves as a venue for people in chronic pain to exhibit their artworks, thereby communicating their pain through art. (The site also serves as an educational resource for the teaching of chronic pain for use by the academic and medical communities worldwide).
Discussion
Art-making as a form of self-expression can be empowering; but as a person who lives in chronic pain and with impairments, I feel that the whole concept of art-as-empowerment in the context of pain, suffering and disability is often perceived as a panacea and has become somewhat of an overused cliché. Far from empowered, my reality is that I often feel completely defeated and beaten down by my pain (not to mention judged) in spite of my best efforts to the contrary. I also loathe the old adage, ‘what does not kill us makes us stronger.’ Learning to overcome challenges gives us the confidence needed to rise up to challenges again; however, the ‘challenge’ of chronic pain is that it is exhausting, destroys quality of life, and can lead to depression. That said, I also believe that pain can serve numerous positive purposes. In particular, pain is a powerful and insightful lens through which to examine the human condition. Being in pain can help to cultivate and deepen empathy, compassion, nurturing, community, thoughtfulness, and humility – and chronic pain sufferers routinely demonstrate incredible resilience, resourcefulness, creativity, courage, collaboration, and determination under extremely difficult and discouraging circumstances.
I would also like to respectfully acknowledge that the relationship between pain, art-making, art as a language, and the role of art in socio-political activism is very complex; so simply creating art, in any form, cannot be expected to provide a voice or visual language, produce catharsis, alleviate pain, solve one’s problems, or empower the disenfranchised. Pain is a highly subjective, variable, and individual experience. As such, not every pain sufferer feels the need to find a voice for his or her pain. In fact, silence is a form of resistance. For me, having visual access to the visceral, corporeal, chronic pain sensations of fellow sufferers, albeit online, is an incredibly validating experience. After much reflection, I propose that the ‘cathartic release’ inherent in using art as a language to express pain lies just as much, if not more so, in its reception than in its production and expression. I credit the courage of artists who unabashedly and publicly expose(d) their pain with having inspired me to re-examine and revise my original 2011 collection, Officially Unapologetic. In confronting my pain in much more direct and honest ways, I feel I have found a stronger voice and more accurate language for the communication of my pain, and as a result, I have experienced some catharsis.3

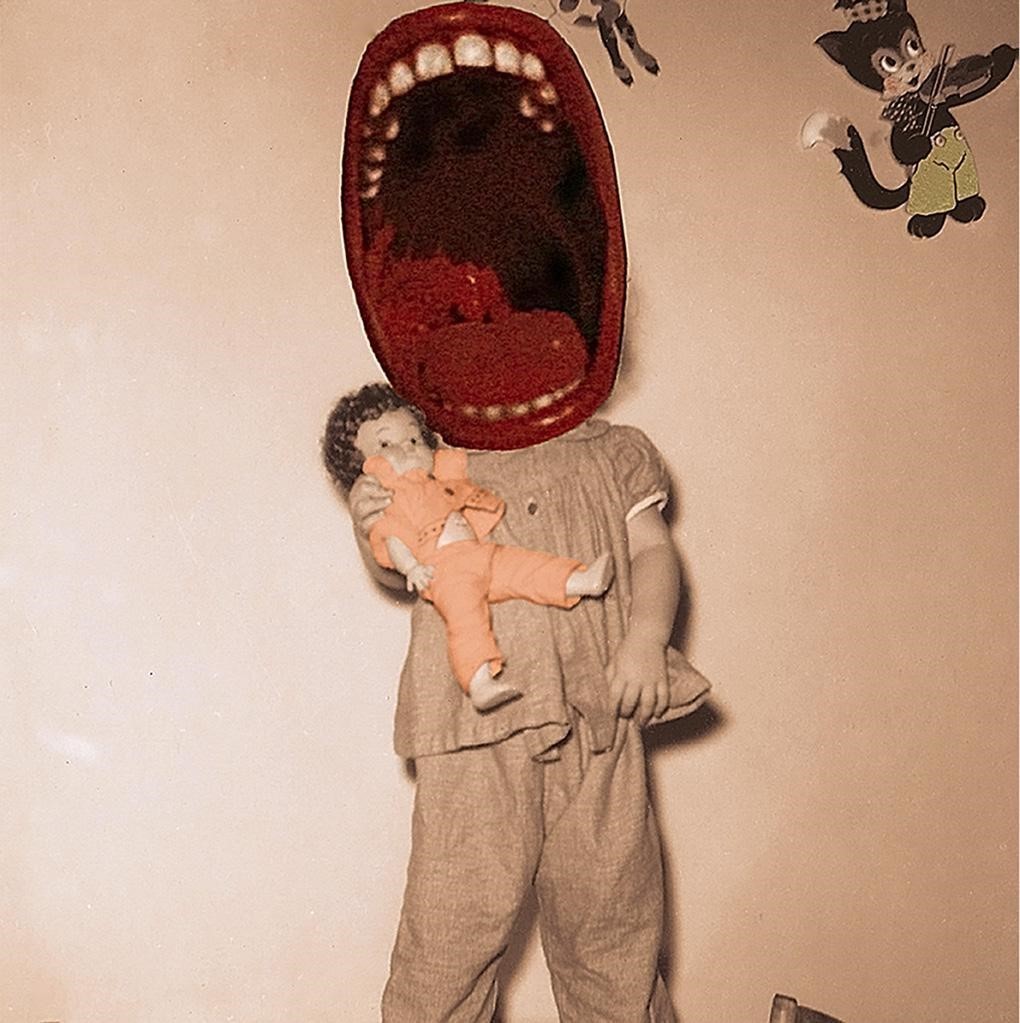
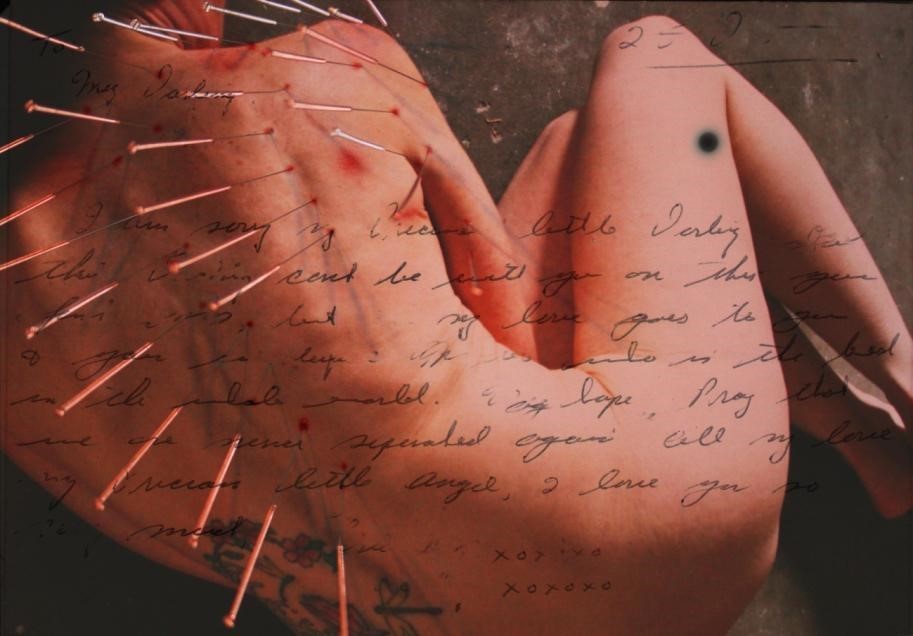
Figure 8: H. Ráine, Self-Portrait – Vultures (from Officially Unapologetic series) 2011 - 2014, Digital Collage

Figure 9: H. Ráine, Self-Portrait – Vultures (from Officially Unapologetic series) 2011 - 2014, Digital Collage
In Conclusion
Most people are naturally narrative beings who are inclined to present and re-present their experiences of the world in order to make sense of their lives and integrate with society (McIntyre in Morris 2001; Coulter-Smith 2000; Ochs and Capps 1996). Experts who theorize about the communication of pain suggest that salvaging or creating meaning from painful experiences is a necessary form of spiritual freedom for some people, and posit that pain can be an invitation to dialogue (Frankl 1984; Jackson 2002). Pain is imbued with meaning that must be communicated in order to be understood; but pain actively and frustratingly shatters language.
Art constitutes a visual language that is not only arresting, but has proven it can successfully bridge the communication gap caused by pain’s silencing effects by either subverting the gaze, generating empathy through the power of the gaze, or by simply providing sufferers with a platform by which to express their suffering – with or without the expectation of catharsis, feedback, commentary, or the knowledge of whether or not one’s message has been seen or heard. With the inception of postmodernism, both disability and pain entered into a new arrangement with narrative. By using performance art, self-portraiture, and performative self-portraiture as visual languages for pain – not to mention the ubiquity of social media such as internet forums, blogs, chatrooms, and video diaries – highly vocalized and publicized representations of the private, intimate body in pain have made their way into the social arena, public sphere, and virtual world. Self-representational images that depict corporeal pain are a highly effective means by which chronic pain sufferers can and do articulate pain and speak the unspeakable when words fail.
Afterword
For those involved in the technological, scientific, and medical fields, failure (otherwise known as research and development) is an integral part of learning through trial and error and building upon mistakes – and an element crucial to success (Ferguson 2014, 68). My story is not intended to imply ‘triumph-over-tragedy.’ Rather, I recognize that if my health and physical capabilities had not so dramatically failed just as I was about to begin the final year of my Bachelor of Fine Arts program, I would not have so blatantly been provided with a research focus, may not have finished my BFA, and certainly would not have been led to undertake a my graduate degree in Equity Studies / Cultural Studies (with a serious focus in Disability Studies). Additionally, being forced to recognize that I have some fairly serious impairments presented me with the opportunity to proudly serve on CUPE BC’s Persons with Disabilities Working Group; and when I serve on other committees within my community, such as those that address poverty and homelessness, I am able to ensure that the perspective of people who live with disabilities is considered. The failure of my health led me out of my comfort zone, mediocrity, and the status quo and into an unknown, alternate direction (albeit, with resistance); but I was able to create a thoughtful and meaningful project and have been provided with a wealth of unanticipated opportunities. I am learning that it is generally easier and more productive to work with one’s ‘failures’ than to try to struggle against them.
Notes
1. The McGill Pain Scale (or McGill Pain Index) was developed by Canadian psychologists Ronald Melzack and Warren Torgerson in 1971. The original Index is a self-report questionnaire designed to provide physicians with descriptions of the quality and intensity of a patient’s pain. After completing the questionnaire, users will have selected seven adjectives that best describe their pain (ie: burning, throbbing, quivering, or flickering). Scarry (2009) notes that any one descriptor, heard in isolation, conveys “very little precise information beyond the general fact that the speaker is in distress” (7); but when certain words are placed in the context of others, a much clearer picture emerges of the sufferer’s sentient, affective, evaluative, and cognitive experience (Ibid., 8).
2. Peter McLaren (2002) describes this process of incorporation as enfleshment (44), and states that refleshment refers to the body’s ability to learn alternate postures and behaviours that break these ingrained habits (Ibid.).
3. Hence the dual dates.
Bibliography
Ahmed, Sara. The Cultural Politics of Emotion. Edinburgh: Edinburgh University Press, 2004.
Bending, Lucy. “Approximation, Suggestion, and Analogy: Translating Pain into Language” The Yearbook of English Studies (2006): 36(1): 131-137.
Burns, Jonathan Kenneth. “Mental Health and Inequity: A Human Rights Approach to Inequality, Discrimination, and Mental Disability.” Health and Human Rights. (2009): 11(2): 19-31.
Cohen, Esther. “The Animated Pain of the Body.” The American Historical Review, 105(1) (Feb. 2000): 36-68.
Coulter-Smith, Graham, ed. The Visual-Narrative Matrix: Interdisciplinary Collisions and Collusions. Southampton, UK: Southampton Institute, 2000.
Detsi-Diamanti, Zoe, Katerina Kitsi-Mitakou and Effie Yiannopoulou, eds. The Future of Flesh: A Cultural Survey of the Body. New York: Palgrave, 2009.
Devereaux, Leslie and Roger Hillman, eds. Fields of Vision: Essays in Film Studies, Visual Anthropology, and Photography. Berkeley: University of California Press, 1995.
Ferguson, M. “Failure Is an Option.” Phi Delta Kappan, 2013, 68-69.
Fox, Broderick, “Shooting Pains” in How does it Feel? Making Sense of Pain. Sternudd, Hans T. and Angela Tumini, eds. (Oxford, UK: Inter-Disciplinary Press, 2011), 17-30.
Frankl, Viktor. Man’s Search for Meaning (Rev. Ed.). New York: Washington Square Press, 1984.
Gladwell, Malcolm. Blink: The Power of Thinking without Thinking. New York: Back Bay Books, 2005.
---. “The Art of Failure.” The New Yorker, August 21, 2000. Accessed March 17, 2015 http://gladwell.com/the-art-of-failure/
Jackson, Marni. Pain: The Fifth Vital Sign. Toronto: Random House, 2002.
Jones, Amelia. “The ‘Eternal Return’: Self Portrait Photography as a Technology of Embodiment.” Signs. 27 (4) (Summer, 2002): 947-978.
Kleinman, Arthur, Veena Das, and Margaret Lock, eds. Social Suffering. Berkeley, CA: University of California Press, 1997.
Levine, Ellen G. and Stephen K. Levine, eds. Art in Action Expressive Arts Therapy. London; Philadelphia: Jessica Kingsley Publishers, 2011.
Lewis, Bradley. “A Mad Fight: Psychiatry and Disability Activism” in The Disability Studies Reader, Lennard J. Davis (New York: Routledge, 2006), 339-352.
McLaren, Peter L. “Critical Performance Pedagogy” in Teaching Performance Studies,
Nathan Stucky and Cynthia Wimmer (Chicago: Southern Illinois University 2002), 41-54.
Melzack, Ronald and Patrick D. Wall. The Challenge of Pain. Harmondsworth: Penguin Books, 1982.
Meyers, Diana Tietjens, ed. Feminists Rethink the Self. Boulder, CO: Westview Press, 1997.
Morris, David B. The Culture of Pain. Berkeley; Los Angeles: University of California Press, 1991.
---. “Narrative, Ethics, and Pain: Thinking with Stories.” Narrative, 9 (1) (Jan., 2001): 55-77.
---. “What We Make of Pain.” The Wilson Quarterly, 18 (4) (Autumn, 1994): 8-26. Naumburg, Margaret. Dynamically Oriented Art Therapy: Its Principles and Practice,
New York: Grune and Stratton, Inc.; Chicago: Magnolia Street Publishers, 1987 [1966]. I am a Perfect Failure, Thank You, Harmony Kaelan Ráine 19
Obourn, Megan. “Audre Lorde: Trauma Theory and Liberal Multiculturalism.” MELUS 30(3) Personal and Political (Fall, 2005): 219-245.
Ochs, Elinor and Lisa Capps. “Narrating the Self.” Annual Review of Anthropology, Vol. 25 (1996): 19-43.
Sacks, Oliver. Migraine. New York: Vintage, 1992.
Scarry, Elaine. The Body in Pain: The Making and Unmaking of the World. New York: Oxford University Press, 1985.
Selzer, Richard. “The Language of Pain.” The Wilson Quarterly, 18 (4) (Autumn, 1994): 28-33.
Semino, Elena. “Descriptions of Pain, Metaphor, and Embodied Simulation.” Metaphor and Symbol, 25 (2010): 205–226.
Snyder, Sharon and David T. Mitchell. Cultural Locations of Disability. Chicago: University of Chicago Press, 2006.
Sontag, Susan. Regarding the Pain of Others. New York: Farrar Straus Giroux, 2003.
Spence, Jo. Property of Jo Spence? (from A Picture of Health? series) [image], 1982-1986. Retrieved November 28, 2014 from http://www.jospence.org/picture_of_health
---. Untitled Self-Portrait (from A Picture of Health? series) [image], 1982-1986. Retrieved November 28, 2014 from http://www.jospence.org/picture_of_health
Sturken, Marita and Lisa Cartwright. Practices of Looking: an Introduction to Visual Culture (2nd Ed.). New York: Oxford University Press, 2009.
Sternudd, Hans T. and Angela Tumini, Eds. How does it Feel? Making Sense of Pain. Oxford, UK: Inter-Disciplinary Press, 2011.
Thomson, Rosemarie Garland. Extraordinary Bodies: Figuring Physical Disability in American Culture and Literature. New York: Columbia University Press, 1997.
---. “Integrating Disability, Transforming Feminist Theory” NWSA Journal 14 (3), Feminist Disability Studies (Autumn 2002): 1-32.
Tumini, Angela and Mira Crouch. “Introduction” in How does it Feel? Making Sense of Pain, Hans T. Sternudd and Angela Tumini, eds. (Oxford, UK: Inter-Disciplinary Press, 2011): vii-x.
Wall, Patrick. Pain: The Science of Suffering. New York: Columbia University, 2000.
Wong, Donna and Connie Baker. Wong-Baker FACES Pain Rating Scale [image], 1983. Retrieved December 3, 2014 from www.wongbakerFACES.org




F T I