
- Page Not Found
- Research
- Covid-19 Research
- People
- Software
- Events
- Resources
- Blog
- Fundamental Limitations of Contact Tracing for COVID-19
- After vaccination: What happens next in BC
- High transmission variants: The benefits of being proactive
- Vaccinating essential workers
- Are there COVID variants amongst us?
- What if a high-transmission variant takes off?
- What to expect when schools reopen
- Parks and Bars
- Join Us
Fundamental Limitations of Contact Tracing for COVID-19
P. Tupper, S. Otto, C. Colijn
Contact tracing has played a central role in COVID-19 control in many jurisdictions and is often used in conjunction with other measures such as travel restrictions and social distancing mandates. Contact tracing is made ineffective, however, by delays in testing, calling, and isolating. Even if delays are minimized, contact tracing can only prevent a fraction of onward transmissions from contacts. Without other measures in place, contact tracing alone is insufficient to prevent exponential growth in the number of cases in a population with little immunity. Even when used effectively with other measures, occasional bursts in call loads can overwhelm contact tracing systems and lead to a loss of control. We propose embracing approaches to COVID-19 control that broadly test individuals without symptoms, in whatever way is economically feasible – either with fast cheap tests that can be deployed widely, with pooled testing, or with screening of judiciously chosen groups of high-risk individuals. Only by ramping up testing of asymptomatic individuals can we avoid the inherent delays that limit the efficacy of contact tracing. These considerations are important both in regions where widespread vaccination has been deployed, and in those where still few residents have been immunized.
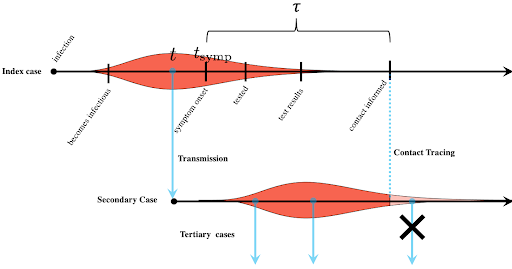
The effectiveness of contact tracing for any infectious disease is limited by how quickly contacts can be informed. If contact tracing teams reach an individual’s contacts only toward the end of their infectious period, very few further infections will be prevented. Several delays in the process make rapid contact tracing challenging: the time to develop symptoms, to seek a test, to get test results, and for contact tracing teams to reach contacts. Contact tracing is particularly challenging for COVID-19 because transmission often occurs before symptoms appear and some individuals can transmit who never develop symptoms at all.
Before the widespread deployment of vaccination, symptomatic testing followed by contact tracing, set in the context of ongoing widespread distancing measures, had been the primary means of controlling COVID-19 in many jurisdictions in Europe, the UK and North America. However, broad and restrictive distancing measures were considered too costly to be palatable in the long term, both economically and in terms of unintended consequences for public health, mental health and inequality. This left most of North America, Europe and the UK, among others, in the position of repeatedly re-opening their economies following periods of declining COVID-19 numbers. This reopening has occurred in a context where COVID-19 immunity was very low, substantial costs had been incurred, but COVID-19 had not been eliminated and/or was continually re-introduced. In many areas, contact tracing capacity was dramatically increased to allow reopening.
After reopening and before vaccination, almost all jurisdictions in North American and Europe saw substantial resurgences of COVID-19 despite having testing and contact tracing in place. Some overwhelmed their health care systems, for example exceeding ICU capacity, cancelling elective surgeries, diverting patients, and being depleted of nursing staff, leading in some cases to health care workers being asked to work while testing positive for COVID-19. Groups of doctors have written open letters calling for wider shutdowns while politicians hesitate, knowing the costs and the unintended damages that these shutdowns will create. This has occurred despite symptomatic testing and contact tracing being in place. It is clear that the level of widespread distancing that is tolerable and sustainable is insufficient for robust COVID-19 control, with the testing and contact tracing systems currently in place.
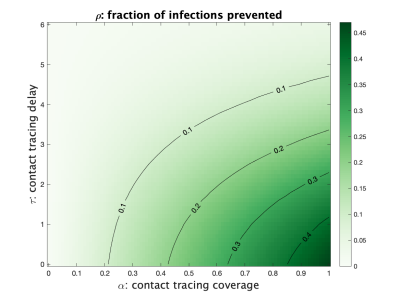
Under normal patterns of social interaction with no contact tracing and no immunity, R for COVID-19 is estimated to be between 2 and 5. Social distancing and other NPIs without the use of contact tracing reduce the basic reproductive number R to some lower value RNCT, the basic reproductive number with no contact tracing. Contact tracing reduces this further to R=(1-ρ) RNCT, where ρ is the fraction of cases a contact would infect that are prevented by contact tracing. This fraction depends on the capacity to contact trace and on the timing of symptoms and transmission. Two important features are the fraction of contacts that can be reached and who self-isolate (we call this fraction α or “coverage”) and the time from a positive test until the contacts are reached (we call this time τ). When cases are rare, contact tracers can rapidly reach a large proportion of a case’s contacts. As the number of cases rises, contact tracing capacity can become increasingly taxed, reducing the ability to reach all contacts and lengthening the delay. In the figure below we illustrate the fraction of cases that contact tracing can prevent given the current tracing capacity, i.e. how ρ depends on α and τ.
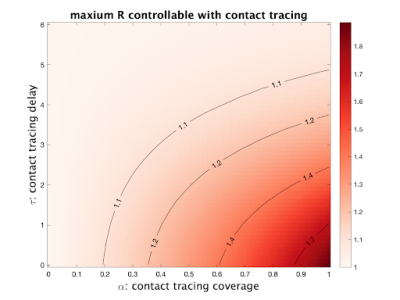
If we already have contact tracing in place, we cannot observe RNCT. But if we have estimates of R, the coverage and the delay, we can estimate RNCT from RNCT = R / (1-ρ).
Then we can determine the fraction of new cases (ρcrit) we would have to prevent to bring R below 1 by solving 1 = (1-ρcrit) RNCT. As an example, in British Columbia, on Nov 1, 2020, we estimate R=1.22 ((1.13,1.35) 90% range), with that τ approximately 5 days in ideal cases (roughly 1 day for symptom onset to test, 2 days for the test result to be available, and another 2 days for the contacts to be notified, though this varies from one to many days. With coverage of α=0.5, our formula yields ρ =0.08 and RNCT= 1.33: contact tracing only prevents 8% of onward cases. To reduce R to 1 we would need ρ = 1- (1/1.33)= 0.25. This could be achieved by reducing delays in contacting from 5 to 2.8 days. Alternatively we could increase coverage, but R is only reduced to 1.12 even if we reached 100% of contacts (α=1), which wouldn't bring spread under control. In reality, a combination of decreasing delays (τ) and increasing coverage (α) would be optimal.
The fact that there is a critical value of the contact tracing delay beyond which contact tracing is not able to prevent a sufficient fraction of cases to bring COVID-19 under control is an example of a tipping point: a value of a parameter where a system has qualitatively different behaviour when the parameter is above or below it. If the delay τ is above its critical value, we have exponential growth in the number of cases; otherwise cases decline. There is another tipping point for the coverage; increasing coverage (for example by expanding the definition of a contact to include more people, taking extra measures to insure compliance with self-isolation) could push R below 1 if τ is sufficiently short and other measures are in place.
Without extensive distancing or any immunity in the population, contact tracing with realistic parameters will not be able to bring R below 1 and we will have exponential growth in the number of cases. But the situation will become worse even for initially very mild exponential growth. As the number of incident cases increases, the contact tracing system will be put under a heavier load, with both τ increasing and α decreasing, meaning an even lower fraction of cases are prevented by contact tracing. R increases even further, which in turn causes even faster growth in the number of incident cases. This positive feedback cycle unabated will lead to the contact tracing system being overwhelmed, since contact tracing capacity cannot be expanded as quickly as case numbers rise.
If a region does have COVID cases under control (R<1), we can also determine how large an increase in call load can be handled before contact tracing will fail to limit spread. As the number of individuals who need to be contacted daily (n) rises above the tracing capacity (c), the best strategy is to reduce coverage without also adding further delays. In this case, coverage will decline in proportion to how far over capacity the call demand is (e.g., coverage will drop by half if twice as many people need to be called as can be called, n/c=2). Solving for the call volume that will cause R to rise above one, we find that contact tracing breaks down once n/c > ρ RNCT/(RNCT-1) or, equivalently, n/c > (RNCT-R)/(RNCT-1). For example, in a region brought down to R=0.9 from RNCT=1.33, contact tracing will fail to prevent spread once the demand requires 33% more calls than can be placed in a day.
This is the best case scenario - only coverage was impacted. In reality, as the incidence or call volume rises, delays grow. Testing backs up so that fewer onward cases can be prevented. Thus, any event -- a burst in transmission caused by a superspreading event, a cluster of importations, or changes in behaviour around a holiday -- that causes the call volume to rise above this limit cannot be reversed by contact tracing alone. Importantly, the number of calls needed can rise either because of true increases in incidence or due to increases in contacts per case -- either can cause this kind of collapse. When cases rise, the effectiveness of contact tracing declines just when it is most needed.
Where does this leave us? In regions where there is little immunity either through vaccination or infection, health authorities must face up to the fact that they cannot have what they so wanted -- considerable reopening to avert the high costs of shutdowns -- if their primary COVID-19 controls are based on symptomatic testing and contact tracing. Either strong distancing measures must be maintained until a vaccine has been widely deployed, or we must rethink our testing and tracing approach. One option for considerably strengthening the power of contact tracing is to go beyond merely instructing contacts to isolate, but to test all contacts of a known case as rapidly as possible, whether or not they are symptomatic. This approach, which is used in New Zealand, has the advantage that if a secondary contact tests positive, tracing for their contacts can be initiated much earlier than if testing only occurs after symptom onset, which might never happen if the secondary contact remains asymptomatic. In contrast, if we simply ask individuals to self-isolate, first this isolation is imperfect, and we do not obtain information about their contacts early enough to prevent onward transmission from them.
Mass testing is another approach recently used in Slovakia, where two thirds of the country were tested with rapid antigen tests over two days. 57,500 COVID-19 cases were identified, which is almost three quarters the number of cases discovered by PCR tests in that country since the beginning of the pandemic. These tests are less accurate than standard PCR tests, but lower cost means that they can be deployed much more widely. Pooled sample testing is another approach: samples are collected from a group and tested at once, reducing the costs of testing. A positive result can lead to instructions to isolate for the whole group and/or to subsequent individual tests. In addition, when call load exceeds contact tracing capacity in a region, mass testing and isolation of positive cases could be used to bring case numbers down to where contact tracing would become effective again. What these have in common is that they aim to find cases, and even contacts of those cases, before symptom onset, at the start of or before infectiousness (effectively reducing τ). Measures initiated by testing symptomatic individuals cannot “get ahead of transmission” in the same way.
We can either find ways to get ahead of transmission or continue to use symptomatic testing followed by contact tracing as our primary COVID-19 control. But we now know that (in the absence of vaccination) contact tracing that focuses on symptomatic cases must be complemented with long, sustained and widespread distancing measures, and these have extremely high economic, social and health costs. If we want to avoid continual shutdowns and resurgences, we need to build robust testing strategies and capacity that can stop transmission much earlier.
Now that vaccines are approved and are being widely deployed, and vaccinated populations are moving to reopen economic and social activities, testing and contact tracing will face new challenges. First, people will have a lot more contacts when they are working in person, socializing indoors and travelling more: effectively we are increasing the reproductive number back up towards pre-pandemic levels. Vaccination will counteract this rise, preventing a large fraction of infections and providing good protection against symptomatic disease, as infections in vaccinated individuals appear to be more often asymptomatic. The relative transmissibility per unit time is not known, but asymptomatic individuals will not know that they are infectious unless they are tested, so they will likely circulate (and have contacts) for longer times than symptomatic individuals have done under social distancing during the pandemic. This poses challenges for identifying an individual’s infector, though it does mean that if an individual is identified early in their infection, there is an opportunity to prevent a high portion of their onward transmission. It poses challenges for testing, as the contacts of a case may also be asymptomatic with higher probability due to vaccination. This means that in order for contact tracing to succeed it may need to rely more on testing asymptomatic contacts, and its effectiveness may be undermined as we reopen by large numbers of potential contacts, reduced interest in testing, and assumptions that vaccinated individuals are not infected or infectious. Contact tracing needs to be reassessed and adjusted once we know more about COVID-19 transmission in a largely immunized population.